A Comprehensive Guide to Patellofemoral Pain Syndrome
Introduction
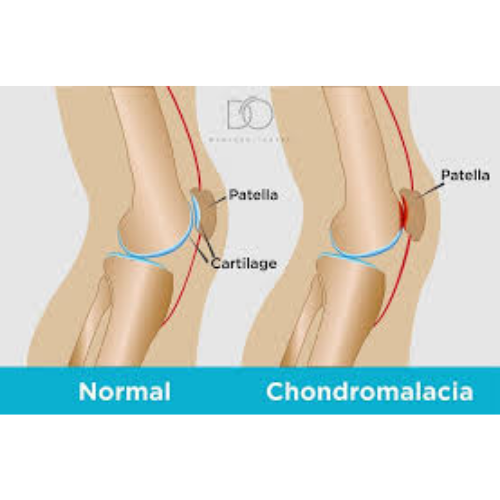
Chondromalacia patellae, also known as runner’s knee or patellofemoral pain syndrome, refers to the softening and breakdown of the cartilage on the underside of the kneecap (patella). This common condition affects people of all ages, particularly active individuals and young adults. Understanding the causes, symptoms, and treatment options can help you effectively manage this condition and maintain an active lifestyle.
What Is Chondromalacia Patellae?
The patella (kneecap) is covered with smooth articular cartilage that allows it to glide smoothly in a groove at the end of the femur (thigh bone). In chondromalacia patellae, this cartilage becomes softened, roughened, or damaged. The condition is graded by severity from grade one (mild softening) to grade four (exposed bone with complete cartilage loss).
The damage occurs when abnormal forces act on the patellofemoral joint, typically due to malalignment, muscle imbalances, or overuse. Over time, this leads to cartilage degeneration, inflammation, and pain.
Causes and Risk Factors
Biomechanical Factors
Several structural and alignment issues predispose to chondromalacia including patellar malalignment or maltracking where the kneecap doesn’t track properly in its groove, muscle imbalances with weak quadriceps (especially the vastus medialis oblique), tight hamstrings, iliotibial band, or hip flexors, flat feet or overpronation causing altered lower extremity mechanics, and hip weakness leading to femoral internal rotation and knee valgus.
Activity-Related Causes
Certain activities and training errors contribute including overuse from repetitive knee flexion activities, sudden increases in training intensity or duration, running on uneven surfaces or excessive downhill running, sports involving jumping, cutting, or pivoting, and poor athletic technique or form.
Anatomical Factors
Some individuals have predisposing anatomy including shallow femoral groove (patella alta), abnormal Q-angle (the angle between quadriceps and patellar tendon), genu valgum (knock-knees) or genu varum (bow legs), and femoral or tibial torsion.
Other Risk Factors
Additional factors that increase risk include previous knee injury or trauma, adolescence and growth spurts, female gender (due to wider pelvis and resultant biomechanics), obesity increasing joint loading, and genetic predisposition.
Signs and Symptoms
Primary Symptoms
The characteristic presentation of chondromalacia includes anterior knee pain (front of the knee) that worsens with activities loading the patellofemoral joint. Pain is typically described as aching or grinding, worse with specific activities including climbing or descending stairs (especially down), squatting or kneeling, sitting for prolonged periods with bent knees (“theater sign”), running or jumping, and deep knee bending.
Associated Symptoms
Additional symptoms may include crepitus (grinding, crackling, or popping sensation with knee movement), knee stiffness after prolonged sitting, sensation of knee giving way or instability, mild swelling around the kneecap, and pain when pressing on the kneecap.
Symptom Patterns
Pain patterns provide diagnostic clues. The pain is typically worse at the beginning of activity, may improve with warm-up then return with continued activity, and worsens after activity or the following day. Morning stiffness is common, and symptoms often fluctuate based on activity levels.
Diagnosis
Clinical Examination
Diagnosis is primarily clinical based on history and physical examination. Key examination findings include pain with patellar compression (pressing the kneecap into the groove), pain with patellar tracking (Clarke’s sign), tenderness around the kneecap borders, positive apprehension test if patellar instability present, assessment of patellar mobility and tracking, and evaluation of lower extremity alignment and muscle flexibility.
Imaging Studies
X-rays help evaluate patellar alignment, joint space, and rule out other conditions. They may show patellar tilt or subluxation and degenerative changes in advanced cases. MRI is sometimes used to assess cartilage damage severity, rule out other pathology like meniscal tears, and evaluate for patellar instability factors. CT scan may assess patellar tracking and alignment in complex cases.
Grading System
Chondromalacia is graded arthroscopically or by MRI. Grade 1 shows softening of the cartilage. Grade 2 has fibrillation and fissuring. Grade 3 presents deep fissures and exposed bone in places. Grade 4 has extensive cartilage loss with bone-on-bone contact. Early grades are more responsive to conservative treatment.
Non-Surgical Treatment
The vast majority of chondromalacia cases improve with conservative management. Treatment should be comprehensive and address underlying causes.
Rest and Activity Modification
Initial management includes relative rest from aggravating activities, avoiding or modifying painful activities (stairs, squatting), switching to low-impact activities (swimming, cycling), and gradual return to activity with proper progression.
Physical Therapy
Physical therapy is the cornerstone of treatment focusing on strengthening the quadriceps, particularly vastus medialis oblique (VMO), hip abductor and external rotator strengthening, stretching tight muscles (hamstrings, IT band, hip flexors, calves), improving patellar mobility and tracking, and correcting movement patterns and biomechanics.
Specific Exercises
Effective exercises include straight leg raises, quad sets, short-arc quads, wall sits with proper alignment, step-ups and step-downs with control, clamshells and hip abduction exercises, hip extension exercises, and stretching routines. Exercises should be pain-free or cause minimal discomfort.
Patellar Taping and Bracing
McConnell taping can temporarily improve patellar tracking and reduce pain, allowing better exercise tolerance. Patellar stabilizing braces with lateral buttress may help some patients. Knee sleeves provide compression and warmth. These are adjuncts to, not replacements for, strengthening.
Orthotics and Footwear
For those with overpronation or flat feet, custom or over-the-counter orthotics can improve lower extremity alignment. Proper athletic shoes with adequate support and cushioning are important. Replace worn shoes regularly.
Medications
Over-the-counter NSAIDs help manage pain and inflammation short-term. Acetaminophen provides pain relief. Topical anti-inflammatory creams may benefit some patients. Medications should complement, not replace, physical therapy.
Ice and Heat Therapy
Apply ice after activities for 15 to 20 minutes to reduce inflammation and pain. Heat before activities may help with stiffness. Avoid prolonged icing.
Weight Management
For overweight individuals, weight loss reduces stress on the patellofemoral joint significantly. Even modest weight reduction can provide substantial symptom improvement.
Advanced Non-Surgical Treatments
If conservative measures fail after several months, additional options include:
Injections
Corticosteroid injections may provide temporary relief for significant inflammation, though repeated injections should be avoided. Hyaluronic acid (viscosupplementation) shows mixed results for patellofemoral arthritis. Platelet-rich plasma (PRP) is being investigated but remains controversial.
Alternative Therapies
Some patients benefit from acupuncture, massage therapy targeting surrounding muscles, and dry needling for trigger points. Evidence varies for these modalities.
Surgical Treatment
Surgery is rarely needed and reserved for cases that fail extensive conservative treatment (typically six to 12 months) and have significant cartilage damage.
Arthroscopy
Diagnostic and therapeutic arthroscopy allows direct visualization of cartilage damage, debridement (smoothing) of damaged cartilage, removal of loose bodies, and evaluation of tracking. Benefits are variable and often temporary.
Lateral Release
For documented lateral patellar tilt or excessive lateral tracking, arthroscopic lateral release cuts the tight lateral retinaculum. This is performed less commonly now as outcomes are unpredictable.
Realignment Procedures
For significant malalignment, procedures include tibial tubercle transfer (moving the attachment of the patellar tendon), trochleoplasty (reshaping the femoral groove), and medial patellofemoral ligament reconstruction. These are major procedures for severe cases.
Cartilage Restoration
For focal cartilage defects, options include microfracture to stimulate cartilage regrowth, autologous chondrocyte implantation (ACI), and osteochondral autograft or allograft transplantation. These are specialized procedures for specific indications.
Patellectomy
Removal of the kneecap is a last resort for severe cases unresponsive to all treatments. It significantly weakens the knee and is rarely performed.
Recovery and Prognosis
Conservative Treatment Outcomes
Most patients improve significantly with proper conservative treatment. Improvement typically begins within weeks, with continued gains over three to six months. Some may require ongoing maintenance exercises.
Factors Affecting Outcomes
Better outcomes occur with early treatment initiation, mild to moderate cartilage damage, good compliance with physical therapy, addressing underlying biomechanical issues, and appropriate activity modifications.
Surgical Outcomes
Surgical results are more variable and depend on the procedure, severity of damage, and patient selection. Recovery from arthroscopy takes several weeks, while realignment procedures require months.
Long-Term Management
Chondromalacia is often a chronic condition requiring ongoing management including continued strengthening and stretching exercises, activity modifications as needed, maintaining healthy weight, and proper footwear and orthotics if needed.
Prevention Strategies
For Athletes and Active Individuals
Prevent chondromalacia or recurrence through gradual training progression avoiding sudden increases, proper warm-up and cool-down routines, cross-training to avoid overuse, strengthening core and lower extremity muscles, maintaining flexibility, proper technique and form in sports, and adequate rest and recovery.
General Prevention
Additional preventive measures include maintaining healthy weight, wearing appropriate footwear, addressing flat feet or overpronation, strengthening quadriceps and hip muscles, and avoiding prolonged sitting with bent knees.
Activity Modifications and Adaptations
Safe Exercises
Low-impact activities that are generally well-tolerated include swimming and water aerobics, cycling (with proper seat height), elliptical machines, yoga and Pilates (modifying poses as needed), and walking on level surfaces.
Activities to Modify or Avoid
Approach these activities cautiously or avoid if they cause pain: running (especially downhill or on uneven terrain), deep squatting or lunges, jumping and plyometrics, climbing or descending stairs repeatedly, and kneeling.
Exercise Guidelines
When exercising, avoid activities causing sharp pain, modify range of motion to pain-free ranges, strengthen in positions that don’t load the patellofemoral joint excessively, and progress gradually as symptoms improve.
When to Seek Medical Attention
Consult an orthopedic specialist if symptoms persist despite conservative treatment for six to eight weeks, pain significantly interferes with daily activities, there is significant swelling or effusion, mechanical symptoms develop (locking, catching), or the knee gives way frequently.
Living with Chondromalacia
Daily Life Adaptations
Managing chondromalacia in daily life includes using handrails on stairs, taking stairs slowly and controlled, avoiding prolonged sitting with bent knees, using cushions to elevate knees slightly when sitting, and modifying work positions if needed.
Maintaining Quality of Life
Most people with chondromalacia can maintain active lifestyles with appropriate modifications. Stay active with low-impact exercises, maintain strengthening and flexibility programs, listen to your body and rest when needed, and adjust activities based on symptoms.
Support and Resources
Consider physical therapist guidance for personalized program development, orthopedic follow-up for persistent symptoms, support groups for chronic pain management, and educational resources about knee health.
Conclusion
Chondromalacia patellae is a common and usually manageable condition. While it can cause significant discomfort and activity limitations, most patients improve substantially with appropriate conservative treatment. The key to success lies in comprehensive rehabilitation addressing muscle imbalances, biomechanical issues, and activity modifications. Physical therapy, particularly quadriceps and hip strengthening, forms the foundation of treatment. Patience and consistency with exercises are essential, as improvement typically takes weeks to months.
Surgery is rarely necessary and reserved for severe cases that fail extensive conservative management. Even then, outcomes are variable. With proper treatment and ongoing maintenance, most individuals with chondromalacia can return to desired activities and maintain good quality of life. Early intervention and addressing contributing factors provide the best outcomes. If you experience persistent anterior knee pain, consult with an orthopedic specialist or sports medicine physician for proper evaluation and treatment planning. Understanding your condition and actively participating in your rehabilitation offers the best chance for long-term success.