Introduction
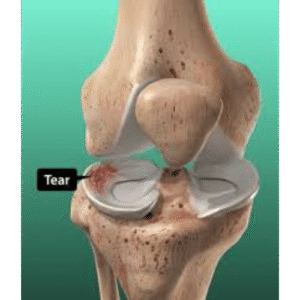
Meniscal tears are among the most common knee injuries, affecting people of all ages from athletes to the elderly. The meniscus is crucial for knee function, acting as a shock absorber and load distributor. Understanding the different types of tears, treatment options, and expected outcomes is essential for making informed decisions about your care. This comprehensive guide will help you navigate this common but often complex condition.
Understanding the Meniscus
Anatomy and Function
Structure:
– C-shaped fibrocartilage structures
– Two per knee: medial (inner) and lateral (outer)
– Wedge-shaped in cross-section
– Attached to tibia (shin bone) at anterior and posterior horns
Key Functions:
– Shock absorption: Absorbs 30-50% of weight-bearing loads
– Load distribution: Spreads forces across joint surface
– Joint stability: Provides secondary stabilization
– Lubrication: Aids in joint fluid distribution
– Proprioception: Provides sensory feedback for joint position
Blood Supply:
– Outer third (red zone): Good blood supply from peripheral vessels
– Middle third (red-white zone): Transitional vascularity
– Inner third (white zone): Avascular (no blood supply)
Clinical Significance: Blood supply determines healing potential. Peripheral tears can heal; inner tears cannot.
Differences Between Medial and Lateral Meniscus
Medial Meniscus:
– More commonly torn (2:1 ratio compared to lateral)
– Less mobile (firmly attached to joint capsule)
– C-shaped
– Attached to medial collateral ligament (MCL)
– More vulnerable to injury
Lateral Meniscus:
– More mobile
– More O-shaped (covers larger area)
– Not attached to lateral collateral ligament (LCL)
– Less commonly torn
– When torn, often associated with ACL injury
Types and Classification of Meniscal Tears
Classification by Pattern
Vertical Tears
Vertical Longitudinal (Bucket Handle):
– Vertical tear running along length of meniscus
– Inner fragment can displace (“bucket handle”)
– May cause locking if displaced
– Often repairable if peripheral
– Common in younger, active patients
Radial Tears:
– Perpendicular to the long axis
– Extends from inner edge toward periphery
– Disrupts circumferential fibers (critical for load distribution)
– Generally not repairable
– Common in middle-aged and older patients
– Severely compromises meniscal function
Vertical Flap Tears:
– Vertical tear with flap that can flip
– May cause mechanical symptoms
– Variable repairability
Horizontal Tears
Horizontal Cleavage:
– Splits meniscus into upper and lower portions
– Common in degenerative menisci
– Often in middle-aged and older patients
– Generally not repairable
– May be stable and asymptomatic
Complex Tears
Complex/Degenerative:
– Multiple tear patterns combined
– Irregular, frayed edges
– Common in older patients
– Usually not repairable
– Indicative of degenerative process
Other Patterns
Root Tears:
– Detachment of meniscus from bone insertion
– Medial root more commonly torn
– Functionally equivalent to total meniscectomy if untreated
– Can be repaired surgically
Parrot Beak/Flap Tears:
– Oblique tear creating a flap
– Can cause catching or locking
– Variable repairability
Classification by Tear Location
Anterior Horn: 5-10% of tears
Body: 10-15% of tears
Posterior Horn: 75-80% of tears (most common)
Classification by Tear Zone
Zone 1 (Red-Red Zone):
– Outer third with good blood supply
– Best healing potential
– Excellent candidates for repair
Zone 2 (Red-White Zone):
– Middle third with moderate blood supply
– Fair healing potential
– May be repairable with augmentation
Zone 3 (White-White Zone):
– Inner third, avascular
– Poor/no healing potential
– Generally not repairable
Causes and Risk Factors
Acute (Traumatic) Tears
Mechanisms:
– Twisting motion with foot planted
– Deep squatting with rotation
– Direct blow to knee
– Sudden pivoting movements
– Hyperflexion or hyperextension
Common Scenarios:
– Sports (football, basketball, soccer, skiing)
– Getting in/out of low car
– Squatting activities
– Kneeling and rising
– Often associated with audible “pop”
Risk Factors:
– Young, active individuals
– Participation in cutting/pivoting sports
– Often occur with ACL tears (30-50% of ACL tears have meniscal tear)
Degenerative Tears
Mechanism:
– Gradual wear and tear over time
– No specific injury often
– Accumulated microtrauma
– Age-related changes in meniscal tissue
Characteristics:
– Horizontal or complex tear patterns
– Frayed, irregular edges
– Often asymptomatic initially
– Commonly associated with early arthritis
Risk Factors:
– Age >40 years
– Obesity
– Occupations requiring squatting/kneeling
– Previous knee injury
– Family history
– Malalignment (bow-legged or knock-kneed)
Signs and Symptoms
Acute Traumatic Tears
Immediate Symptoms:
– Sudden knee pain (often joint line)
– Audible “pop” sometimes
– Immediate swelling (gradual over 24 hours)
– Difficulty bearing weight
– Pain with twisting or pivoting
– Inability to fully straighten knee (if locked)
Ongoing Symptoms:
– Catching or locking sensation
– Giving way feeling
– Stiffness, especially after sitting
– Difficulty squatting or kneeling
– Pain with stairs (especially down)
Degenerative Tears
Presentation:
– Gradual onset of symptoms
– May not recall specific injury
– Intermittent pain and swelling
– Pain along joint line
– Stiffness in morning
– Symptoms worsen with activity
– May have periods of no symptoms
Physical Examination Findings
Inspection:
– Possible swelling (effusion)
– Muscle atrophy if chronic (quadriceps)
– No obvious deformity typically
Palpation:
– Joint line tenderness (90% sensitivity)
– Medial or lateral depending on tear location
– Pain at specific point along joint line
Range of Motion:
– May be limited by pain or mechanical block
– Pain at end range flexion or extension
– True locking (cannot fully extend) suggests displaced tear
Special Tests:
McMurray Test:
– Knee flexed, foot rotated, knee extended while applying valgus/varus stress
– Positive if pain or clicking at joint line
– 60-70% sensitivity
Apley Grind Test:
– Patient prone, knee bent 90 degrees
– Downward pressure applied while rotating foot
– Positive if pain produced
– 60-70% sensitivity
Thessaly Test:
– Patient stands on one leg, knee slightly bent (20 degrees)
– Rotates body side to side
– Positive if pain at joint line
– Higher sensitivity (75-90%)
Limitations: No single test is 100% accurate; combination of history, exam, and imaging needed.
Diagnosis
Clinical Diagnosis
History:
– Mechanism of injury (or lack thereof)
– Character of pain
– Mechanical symptoms (locking, catching)
– Functional limitations
– Previous knee problems
Physical Examination:
– As described above
– Assess for associated injuries (ACL, MCL)
– Evaluate for arthritis
Imaging Studies
X-rays (Standard First Test)
Purpose:
– Rule out fracture
– Assess for arthritis
– Evaluate alignment
– Check for loose bodies
Views:
– AP (anteroposterior)
– Lateral
– Skyline (patella)
– Weight-bearing if assessing arthritis
Limitations:
– Cannot see meniscus directly
– Only shows indirect signs
MRI (Gold Standard for Meniscal Tears)
Accuracy:
– Sensitivity: 85-95%
– Specificity: 85-95%
– Best non-invasive test
Provides Information On:
– Tear location and pattern
– Tear size and extent
– Associated injuries (ACL, cartilage, bone bruising)
– Degenerative changes
– Cyst formation
MRI Appearance:
– Grade 1: Increased signal not extending to surface (normal or degeneration)
– Grade 2: Increased signal not extending to surface (degeneration)
– Grade 3: Increased signal extending to surface (TRUE TEAR)
Limitations:
– False positives (degenerative signal may look like tear)
– False negatives (small tears may be missed)
– Cannot assess stability of tear
– Expensive
Ultrasound
Advantages:
– Dynamic assessment
– No radiation
– Cost-effective
– Point-of-care
Limitations:
– Operator dependent
– Cannot see entire meniscus
– Less accurate than MRI (70-80%)
– Better for peripheral tears
Arthroscopy (Definitive Diagnosis and Treatment)
Gold Standard:
– Direct visualization
– 100% accuracy
– Allows simultaneous treatment
– Can assess stability and repairability
When Used:
– Diagnostic uncertainty
– Treatment planning
– During surgery
Treatment Options
Decision Making Factors
Patient Factors:
– Age and activity level
– Symptoms and functional limitations
– Occupation and goals
– Willingness to undergo surgery and rehabilitation
– Medical comorbidities
Tear Factors:
– Type and pattern
– Location and size
– Acute vs degenerative
– Associated arthritis
– Mechanical symptoms (locking)
General Approach:
– Acute tears in young patients: More likely surgical
– Degenerative tears in older patients: Often conservative initially
– Locked knee: Urgent surgery needed
– Minimal symptoms: Conservative approach
Conservative (Non-Surgical) Treatment
Indications:
– Small, stable tears
– Degenerative tears in older patients
– Minimal symptoms
– No mechanical symptoms
– Concurrent arthritis (surgery may not help)
– Patient preference
Components:
1. Activity Modification
Avoid:
– Deep squatting
– Kneeling
– Twisting/pivoting activities
– High-impact activities
– Sports temporarily
Allowed:
– Walking
– Swimming
– Cycling (elevated seat)
– Elliptical
– Water aerobics
2. Medications
NSAIDs:
– Ibuprofen, naproxen
– Reduces pain and inflammation
– Take with food
– 2-4 weeks typically
Acetaminophen:
– For pain relief
– No anti-inflammatory effect
– Safer for stomach
Topical:
– Diclofenac gel
– Ice packs
3. Physical Therapy (Key Component)
Duration: 6-12 weeks, 2-3 times/week
Goals:
– Reduce pain and swelling
– Restore range of motion
– Strengthen muscles (especially quadriceps)
– Improve function
Exercises:
Range of Motion:
– Heel slides
– Prone knee flexion
– Wall slides
– Full extension critical
Strengthening:
– Straight leg raises (4 directions)
– Mini squats (limited depth)
– Step-ups
– Leg press (limited ROM)
– Hamstring curls
– Hip strengthening
Proprioception:
– Balance exercises
– Single leg stance
4. Injections
Corticosteroid Injection:
– Reduces inflammation
– Provides temporary relief (weeks to months)
– May help determine if symptoms from meniscus vs arthritis
– Limited to 3-4 per year
Hyaluronic Acid (Viscosupplementation):
– Series of 3-5 injections
– More beneficial for arthritis than meniscal tear
– May provide 6-12 months relief
– Variable insurance coverage
**PRP (Platelet-Rich Plasma):**
– Experimental for meniscal tears
– Limited evidence
– Expensive, not typically covered
5. Bracing
Unloader Brace:
– For degenerative tears with arthritis
– Shifts load away from damaged area
– May reduce symptoms
– Particularly if malalignment present
Success of Conservative Treatment
Studies Show:
– 40-60% of patients improve with conservative treatment
– Better results with:
* Degenerative tears
* Older patients
* Stable tears
* Minimal mechanical symptoms
– May take 3-6 months to see maximum benefit
– Some eventually require surgery
Trial Period:
– Usually 6-12 weeks of conservative treatment
– Re-evaluate if not improving
– Consider surgery if:
* Persistent symptoms affecting quality of life
* Mechanical symptoms (locking, catching)
* Failed aggressive non-operative treatment
Surgical Treatment
Indications:
– Failed conservative treatment (6-12 weeks minimum in most cases)
– Mechanical symptoms (locking, catching)
– Significant functional limitation
– Young, active patient with repairable tear
– Acute large tear in healthy meniscus
– Bucket handle tear with displacement
Surgical Options:
1. Partial Meniscectomy (Most Common)
Procedure:
– Arthroscopic (minimally invasive)
– 2-3 small incisions
– Remove torn, unstable portion
– Preserve as much healthy meniscus as possible
– Outpatient procedure
– 30-45 minutes typically
Recovery:
– Weight bearing immediately with crutches for comfort
– Return to desk work: 3-7 days
– Return to sports: 4-6 weeks
– Full recovery: 6-12 weeks
Success Rate:
– 75-90% good to excellent results
– Better outcomes in younger patients
– Less successful if significant arthritis present
Long-Term Considerations:
– Loss of meniscal tissue increases arthritis risk
– Studies show increased arthritis 10-20 years later
– Risk proportional to amount removed
2. Meniscal Repair
Indications:
– Peripheral tear (red-red or red-white zone)
– Vertical longitudinal tear pattern
– Acute tear (<6-12 months)
– Young patient (<40 years typically)
– Good tissue quality
– Length >1 cm
– Concurrent ACL reconstruction
Procedure:
– Arthroscopic typically
– Tear sutured back together
– Various techniques (inside-out, outside-in, all-inside)
– Requires protection during healing
Recovery: (See separate article on meniscal repair recovery)
– Protected weight bearing 4-6 weeks
– Brace typically 4-6 weeks
– Return to sports: 5-6 months
– Much longer than meniscectomy
Success Rates:
– Overall: 70-90% healing rate
– Peripheral tears: 85-95%
– With ACL reconstruction: 90-95%
– Root repairs: 70-85%
Advantages:
– Preserves meniscus
– Reduces long-term arthritis risk
– Better knee biomechanics
Disadvantages:
– Longer recovery
– Risk of retear (10-30%)
– More extensive rehabilitation
3. Meniscal Transplant
Indications:
– Previous total or near-total meniscectomy
– Age <50 typically
– Stable knee (intact ligaments or reconstructed)
– Minimal arthritis
– Persistent pain after meniscectomy
– Failed other treatments
Procedure:
– Donor meniscus (allograft)
– Implanted and secured to bone and capsule
– Complex procedure
– Requires precise sizing
Recovery:
– 6-8 weeks non-weight bearing
– 6-12 months full recovery
– Gradual return to activities
Outcomes:
– 65-85% good to excellent at 5 years
– May slow arthritis progression
– Does not restore normal knee
– Long-term durability unclear
4. Root Repair
Special Procedure:
– Reattaches meniscal root to bone
– Uses suture anchors or tunnels
– Critical for preserving meniscal function
– Root detachment = functional meniscectomy
Recovery:
– Similar to meniscal repair
– Protected weight bearing
– 6-9 months to full activities
Outcomes:
– 75-85% good results
– Prevents progression of arthritis
– Better than leaving unrepaired
Special Situations
Meniscal Tear with ACL Tear
Considerations:
– 30-50% of ACL tears have meniscal tear
– Both often addressed in same surgery
– Meniscal repair healing better with ACL reconstruction
– Follow ACL rehabilitation protocol primarily
Meniscal Tear with Arthritis
Complex Decision:
– Surgery may not help if significant arthritis
– Conservative treatment often first choice
– If surgery, set realistic expectations
– May provide temporary relief only
– Consider injection as diagnostic test
Evidence:
– Multiple studies show meniscectomy no better than PT for degenerative tears with arthritis
– Surgery should not be routine for this situation
Discoid Meniscus
Special Variant:
– Abnormally shaped meniscus (disc-shaped vs C-shaped)
– Congenital condition
– 3-5% of population
– More prone to tearing
– May require saucerization (reshaping) if torn
Pediatric and Adolescent Considerations
Special Factors:
– Open growth plates
– Higher healing potential
– Repair attempted more often
– Long-term implications more significant
– Preserve meniscus when possible
Return to Sport/Activity
After Partial Meniscectomy
Timeline:
– Non-impact activities: 2-3 weeks
– Jogging: 3-4 weeks
– Sport-specific training: 4-5 weeks
– Full return to sport: 4-6 weeks
Criteria:
– Full range of motion
– Minimal swelling
– Adequate strength (>80% of opposite leg)
– Sport-specific function testing passed
– Physician clearance
After Meniscal Repair
Timeline: (See full recovery article)
– Non-impact activities: 3-4 months
– Jogging: 4-5 months
– Return to sport: 5-6 months
Criteria:
– Full range of motion
– >90% strength of opposite leg
– No pain or swelling
– Passed functional testing
– Physician clearance
Prevention
Primary Prevention
Risk Reduction:
– Proper warm-up and stretching
– Neuromuscular training programs
– Strength training (quadriceps, hamstrings, hip)
– Plyometric and balance training
– Proper technique in sports
– Appropriate progression of training
– Maintain healthy weight
For Athletes:
– ACL injury prevention programs (also reduce meniscal tear risk)
– FIFA 11+ program
– Proper landing mechanics training
Secondary Prevention (After Injury)
After Meniscectomy:
– Maintain muscle strength
– Weight management
– Low-impact activities
– Monitor for arthritis development
– Consider viscosupplementation if arthritis develops
After Repair:
– Follow rehabilitation protocol strictly
– Gradual return to activities
– Maintain strength and flexibility
– Protect knee from reinjury
Prognosis and Long-Term Outlook
After Meniscectomy
Short-Term:
– 75-90% good to excellent results
– Significant pain relief
– Return to activities
Long-Term:
– Increased arthritis risk
– Risk correlates with amount removed
– 10-20 years: 20-50% develop arthritis
– Larger amounts removed = higher risk
After Meniscal Repair
Short-Term:
– 70-90% successful healing
– Longer recovery than meniscectomy
– Risk of retear (10-30%)
Long-Term:
– Preserved meniscal function
– Lower arthritis risk than meniscectomy
– Better knee biomechanics
– May last lifetime if heals successfully
Untreated Symptomatic Tears
Risks:
– Progression to larger tears
– Development of cartilage damage
– Increased arthritis risk
– Chronic pain and dysfunction
– Progressive functional limitations
When to See a Doctor
Initial Evaluation:
– Acute knee injury with pain and swelling
– Mechanical symptoms (locking, catching)
– Pain lasting >2 weeks
– Functional limitations
Urgent Evaluation:
– Locked knee (cannot straighten)
– Severe pain and swelling
– Unable to bear weight
– Signs of infection (fever, redness, warmth)
Follow-Up Needed:
– Not improving with conservative treatment after 6-8 weeks
– Recurrent symptoms
– Considering surgical options
– Questions about treatment plan
Conclusion
Meniscal tears are common injuries with a wide spectrum of presentations from acute traumatic tears in young athletes to degenerative tears in older adults. Treatment decisions should be individualized based on tear characteristics, patient age and activity level, symptoms, and goals. While surgical options exist and can be highly effective, conservative treatment should be considered first for many tears, particularly degenerative tears in older patients without mechanical symptoms. When surgery is needed, the goal should be to preserve as much meniscal tissue as possible through repair when feasible. Understanding your specific tear type, treatment options, and expected outcomes will help you make informed decisions with your orthopedic surgeon. Regardless of treatment chosen, maintaining knee strength, flexibility, and healthy body weight will optimize your long-term knee health.