Introduction
Meniscal repair is a surgical procedure to fix torn meniscus cartilage in the knee. Unlike meniscectomy (removal of torn tissue), meniscal repair preserves the crucial shock-absorbing and load-distributing functions of the meniscus. This approach requires a more prolonged and careful rehabilitation to allow the repair to heal. This guide provides comprehensive information about your recovery process.
Understanding Meniscal Tears and Repair
What is the Meniscus?
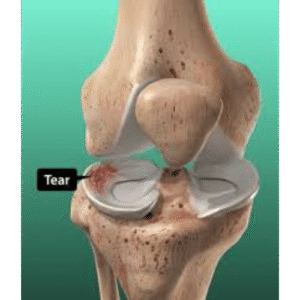
The meniscus is C-shaped fibrocartilage in the knee that:
– Absorbs shock between femur and tibia
– Distributes load across the joint
– Provides stability
– Reduces friction
– Each knee has two: medial (inner) and lateral (outer)
Why Preserve the Meniscus?
Benefits of Repair vs. Removal:
– Preserves natural shock absorption
– Reduces long-term arthritis risk
– Maintains joint mechanics
– Better outcomes for young, active patients
– Protects articular cartilage
Types of Meniscal Tears
Repairable Tears (Best Prognosis):
– Vertical longitudinal tears
– Bucket handle tears
– Peripheral tears in the vascular “red-red” or “red-white” zone
– Acute tears in young patients
Factors Affecting Healing:
– Location: Peripheral heals best (better blood supply)
– Age: Younger patients heal better
– Tear pattern: Simple tears heal better than complex
– Chronicity: Acute tears heal better than chronic
– Associated ACL injury: Healing rates higher with concurrent ACL reconstruction
Recovery Timeline Overview
Important Note: This protocol is for meniscal REPAIR. Meniscectomy (removal) has a much faster recovery (2-4 weeks). Always follow your surgeon’s specific protocol as variations exist.
Standard Timeline:
– Weeks 0-6: Protection phase with limited weight bearing
– Weeks 7-12: Progressive weight bearing and motion
– Weeks 13-16: Strengthening and return to activities
– Months 4-6: Return to unrestricted activities
Phase I: Maximum Protection (Weeks 0-6)
Immediate Post-Operative (Days 0-3)
Goals:
– Protect the repair
– Minimize pain and swelling
– Prevent complications
– Maintain mobility in hip and ankle
Immobilization:
– Knee brace locked in extension (straight)
– Worn 24/7 including sleeping
– May be removed for exercises only
– Duration: 4-6 weeks (varies by surgeon)
Weight Bearing:
– Medial Meniscus Repair: Typically touch weight bearing to partial weight bearing (25-50%)
– **Lateral Meniscus Repair:** May allow more weight bearing (50-75%)
– Use crutches for all ambulation
– No squatting or deep bending
Pain Management:
– Nerve block (12-24 hours)
– Oral pain medications
– Anti-inflammatory medications
– Ice machine or ice packs 20 minutes every 2 hours
– Elevation above heart level
Exercises Begin Day 1:
Ankle Pumps:
– Flex and point foot
– 20 repetitions every hour awake
– Critical for blood clot prevention
Quadriceps Sets:
– Tighten thigh muscle
– Push knee down into bed/brace
– Hold 5 seconds, 10 reps
– Every 2-3 hours while awake
Straight Leg Raises:
– In brace, lift entire leg
– Keep knee straight
– Hold 5 seconds at top
– 10 reps, 3-4 times daily
Gluteal Sets:
– Squeeze buttocks together
– Hold 5 seconds
– 10 reps, 3-4 times daily
Hip Abduction:
– In brace, slide leg out to side
– 10 reps, 3-4 times daily
Weeks 1-2: Early Protection
Goals:
– Continue protecting repair
– Reduce swelling
– Maintain quadriceps activation
– Begin gentle motion (if allowed)
Weight Bearing:
– Continue restricted weight bearing per protocol
– Typically touch to 25-50% body weight
– Progress slowly as directed
Range of Motion (ROM):
– Conservative protocols: Brace remains locked weeks 1-2
– Progressive protocols: May begin gentle passive ROM 0-90 degrees
– Critical: No flexion beyond prescribed limits
– No active knee flexion (hamstring contraction stresses repair)
Permitted Exercises:
Continue from Week 0
Passive ROM (if cleared):
– Heel slides with towel assist
– Gravity-assisted knee flexion (seated, leg hangs)
– Maximum 90 degrees flexion
– 10 reps, 3-4 times daily
Patellar Mobilization:
– Gentle movement of kneecap
– Prevents stiffness
– All directions
– 20 reps, 3 times daily
Wound Care:
– Keep dressing dry until removed (3-5 days)
– May shower once dressing removed
– No submersion (bath, pool, hot tub) until healed (2 weeks)
– Watch for infection signs
Weeks 3-6: Continued Protection with Gradual Motion
Goals:
– Gradually increase weight bearing
– Progress range of motion cautiously
– Continue protecting repair
– Begin gentle strengthening
Weight Bearing Progression:
– Week 3: Progress to 50% weight bearing
– Week 4: Progress to 75% weight bearing
– Week 5-6: Progress to full weight bearing
– Crutches continue until full weight bearing and normal gait
– Wean from two crutches to one to none
Brace:
– Continue locked in extension for walking
– May unlock for exercises if cleared
– Some protocols continue until week 6
– Sleep in brace weeks 0-4, then may discontinue
Range of Motion Goals:
– Week 3: 0-90 degrees (passive)
– Week 4: 0-100 degrees (passive)
– Week 5: 0-110 degrees (passive)
– Week 6: 0-120 degrees (passive and gentle active)
– Extension: Full (0 degrees) by week 2-3
Physical Therapy Begins (typically week 2-3):
– 2-3 times per week
– Focus on ROM and muscle activation
– Patellar mobilization
– Edema control
– Gait training
Exercises Progress:
Passive and Active-Assisted ROM:
– Heel slides
– Wall slides
– Prone knee flexion (gravity assisted)
– Stationary bike with elevated seat (when 110-120 degrees flexion achieved)
Quadriceps Strengthening:
– Quad sets (continue)
– Straight leg raises (4 directions when cleared)
– Short arc quads (30-0 degrees)
– Leg press machine (limited ROM, light weight)
Hip Strengthening:
– Hip abduction (standing or side-lying)
– Hip extension (standing)
– Hip flexion (standing)
– 12-15 reps, 2-3 sets
Balance Activities:
– Single leg stance (on surgical leg)
– Use support initially
– 30 seconds, 5 reps
Restrictions Continue:
– No squatting
– No kneeling
– No pivoting or twisting
– No impact activities
– No resisted knee flexion (hamstring exercises)
Phase II: Intermediate Phase (Weeks 7-12)
Weeks 7-9: Building Foundation
Goals:
– Achieve full weight bearing
– Near-normal range of motion
– Normalize gait pattern
– Progressive strengthening
– Improve proprioception
Weight Bearing:
– Full weight bearing by week 6-8
– Discontinue crutches when:
* Full weight bearing tolerated
* Minimal limping
* Good quadriceps control
Brace:
– Typically discontinued by week 6-8
– May use for stability with walking if needed
Range of Motion Goals:
– Week 9: Full ROM (0-135 degrees) or symmetrical to opposite knee
Exercises Advance:
Stationary Bike:
– Begin when ROM adequate (110-120 degrees)
– Start 10 minutes, no resistance
– Progress to 20-30 minutes
– Add light resistance week 8-9
Leg Press:
– Progress range of motion
– Increase weight gradually
– 60-90 degrees ROM initially
– 12-15 reps, 3 sets
Step-Ups:
– Start with 4-inch step
– Progress to 8 inches
– 12-15 reps, 2-3 sets
Mini Squats:
– Wall support, 0-45 degrees only
– Hold 5 seconds
– 10-12 reps, 3 sets
Leg Curl Machine (Light):
– Very light resistance
– 12-15 reps
– Slowly progress resistance
Balance and Proprioception:
– Single leg stance progression
– Balance board exercises
– Perturbation training
Pool Exercises (when incisions healed):
– Walking in water
– Gentle kicking
– Water provides resistance without impact
Weeks 10-12: Progressive Loading
Goals:
– Continue strength progression
– Improve functional capacity
– Prepare for return to activities
– Achieve strength 70-80% of opposite leg
Advanced Exercises:
Squats:
– Progress depth to 60-90 degrees
– Body weight initially
– Add weight when tolerated
– 10-12 reps, 3 sets
Lunges:
– Forward lunges (small range)
– Lateral lunges
– 10-12 reps each leg, 2-3 sets
Step-Downs:
– Eccentric quadriceps loading
– 8-inch step
– Controlled descent
– 10-12 reps, 3 sets
Wall Sits:
– Hold 30-60 seconds
– Progress to single leg
Hamstring Strengthening (Progressive):
– Leg curls with moderate resistance
– Stability ball hamstring curls
– Nordic hamstring curls (advanced)
– 10-12 reps, 3 sets
Calf Raises:
– Double leg progressing to single leg
– 15-20 reps, 3 sets
Cardiovascular Exercise:
– Stationary bike 30-45 minutes
– Elliptical machine (low impact)
– Swimming (when cleared)
Functional Activities:
– Walking unlimited distances
– Light household activities
– Return to desk work
– Driving (when off narcotics and full weight bearing)
Phase III: Advanced Strengthening (Months 4-5)
Goals:
– Maximize strength and power
– Sport-specific training
– Agility and plyometric training (when appropriate)
– Prepare for full return to activity
Strength Training:
Squat Progressions:
– Full depth squats
– Single leg squats (partial)
– Jump squats (when cleared)
– 10-15 reps, 3-4 sets
Deadlifts:
– Romanian deadlifts
– Single leg deadlifts
– 10-12 reps, 3 sets
Plyometric Exercises (Month 5+):
– Box jumps (start low, 6-12 inches)
– Lateral hops
– Bounding
– Jump rope
– Progress gradually, monitor for swelling/pain
Agility Training:
– Ladder drills
– Cone drills
– Figure-8 running
– Cutting exercises (progressive)
Sport-Specific Training:
– Sport-specific movement patterns
– Interval training
– Position-specific drills
– Simulated game activities
Cardiovascular Progression:
– Walking/hiking
– Jogging program (when cleared, typically month 4-5)
– Cycling
– Swimming
Return to Sport/Full Activity (Months 5-6)
Timeline by Activity Level:
4-5 Months:
– Non-impact recreational activities
– Cycling, swimming
– Golf
– Light recreational sports
5-6 Months:
– Return to running sports
– Basketball, soccer, tennis
– Return to manual labor
– Competitive sports
6+ Months:
– Full unrestricted activity
– Contact sports
– Jumping sports (volleyball, basketball)
Criteria for Return to Sport:
Clinical Criteria:
– Full pain-free range of motion
– No swelling with activity
– Quadriceps strength >90% of opposite leg
– Hamstring strength >90% of opposite leg
– Normal gait pattern
Functional Tests:
– Single leg hop test >90% of opposite leg
– Triple hop test >90%
– Crossover hop test >90%
– Timed hop test >90%
– Y-balance test symmetrical
Clearance:
– Surgeon approval
– Physical therapist approval
– Passed return to sport testing
Sport-Specific Considerations:
Cutting/Pivoting Sports (Basketball, Soccer, Tennis):
– Most challenging for meniscus
– Longer return (6+ months)
– Gradual progression essential
– Proper cutting mechanics critical
Running Sports:
– May return around 5 months
– Gradual mileage build-up
– Monitor for swelling/pain
Contact Sports (Football, Rugby):
– Wait until 6 months minimum
– Full strength and confidence required
– Consider protective bracing
Special Considerations
Root Repairs
– Most conservative protocol
– Extended non-weight bearing (6-8 weeks)
– Slower ROM progression
– May require 6-9 months before sport
Meniscal Transplant
– 6-8 weeks non-weight bearing
– Very gradual progression
– Return to sport 9-12 months
Concurrent ACL Reconstruction
– Follow ACL protocol primarily
– May accelerate meniscal healing (improved vascularity)
– Typically faster return than isolated meniscal repair
Failed Repair (Retear)
– Occurs in 10-30% of cases
– Symptoms: pain, swelling, clicking, locking
– May require revision surgery or meniscectomy
– Higher risk with: complex tears, poor tissue quality, non-compliance
Red Flags – Contact Surgeon
Immediate Attention:
– Sudden sharp pain with “pop” sensation
– Knee locked and cannot straighten
– Severe swelling
– Signs of infection (fever, redness, drainage)
– Inability to bear weight (after initial period)
Schedule Appointment:
– Persistent pain not improving
– Recurrent swelling with activity
– Mechanical symptoms (catching, clicking, locking)
– Feeling of instability
– Unable to progress with therapy
Keys to Successful Recovery
Patient Compliance
– MOST IMPORTANT FACTOR
– Follow weight-bearing restrictions precisely
– Wear brace as instructed
– Don’t rush return to activities
– Non-compliance = high failure rate
Patience
– Healing takes 3-4 months minimum
– Full maturation 6+ months
– Slower than meniscectomy but worth it long-term
– Preserve meniscus = prevent arthritis
Exercise Adherence
– Do prescribed exercises daily
– Quality over quantity
– Attend all PT appointments
– Progress slowly and steadily
Activity Modification
– Avoid squatting and kneeling early phase
– No impact activities until cleared
– Listen to your body
– Some discomfort normal, sharp pain is not
Lifestyle Factors
– Don’t smoke: Impairs healing significantly
– Maintain healthy weight
– Adequate protein intake
– Stay hydrated
– Get sufficient sleep
Communication
– Report all concerns to surgeon/therapist
– Ask questions when unsure
– Honest about pain and activity level
– Discuss return to sport timeline
Long-Term Outlook
Success Rates
– Overall healing rate: 70-90%
– Peripheral tears: 85-95% success
– Inner zone tears: 60-70% success
– With ACL reconstruction: Higher success (90%+)
Factors Predicting Success
– Young age
– Peripheral location
– Acute tear
– Simple tear pattern
– Stable knee (or concurrent ACL repair)
– Patient compliance with protocol
Long-Term Benefits
– Preserved meniscus function
– Reduced arthritis risk
– Better joint mechanics
– Ability to return to high-level activities
Retear Risk
– 10-30% overall
– Higher with non-compliance
– Higher with complex tears
– Monitor for symptoms
Meniscal Repair vs. Meniscectomy
Why Repair Takes Longer:
– Tissue must heal to bone
– Weight bearing stresses repair
– Shear forces with deep flexion
– Blood supply limited
Long-Term Advantages of Repair:
– Preserved shock absorption
– Lower arthritis rates
– Better joint health
– Worth the longer recovery for younger patients
When Meniscectomy is Appropriate:
– Non-repairable tear pattern
– Degenerative tears in older patients
– Failed repair
– Poor tissue quality
Conclusion
Recovery from meniscal repair requires significant patience and adherence to a structured protocol. Unlike meniscectomy, which offers quick return to activity, meniscal repair protects your knee joint for the long term by preserving crucial shock-absorbing tissue. The 5-6 month timeline may seem long, but it’s necessary for proper healing and reduces your risk of arthritis later in life. Follow weight-bearing restrictions meticulously, progress gradually through strengthening phases, and work closely with your rehabilitation team. The vast majority of patients who follow the protocol achieve excellent healing and return to their desired activities, including high-level sports. Your commitment to the recovery process is essential—protecting your meniscal repair now will protect your knee joint for decades to come.